Paul Shapiro MD
Valued member
How Many Grafts Are Needed For a Hair Transplant Surgery?
We've seen common responses when posting Shapiro Medical Group patients on different ht forums. They usually state how good the case looks considering the small number of grafts we use. Here are a few examples I'm referring to:
This is great result for only 2500 grafts
Amazing coverage for the number of grafts Janna.
janna, a very pleasing result with relatively few grafts(considering the area covered)
Wow, Janna! Those results for the # of grafts are amazing, they really are
These comments suggest that there may be a misconception on the number of grafts needed to accomplish a patient s hair transplant goals. I like to think that we use the appropriate amount of grafts for each case taking into consideration the patients goals, donor density, hair caliber, age, degree of balding, family history, response to medical treatment, and the risk/benefit ratio as the cases get larger and go longer.
I would like to point out a few reasons why surgeries using less grafts may lead to the same or very similar results to transplants using greater number of grafts.
1) Each patient has a threshold level of hair density in which their hair will look full under most conditions. Once this threshold is reached as we increase the hair density we get only minimal esthetic improvement. For example let s say a certain patient needs 2,000 FU to reach this threshold level for the area being transplanted. If we transplant 2,500 FU in this area the esthetic improvement will be very similar to planting 2,000 FU. Thus the results of the two transplants could look similar even though in one surgery 500 more FU were planted.
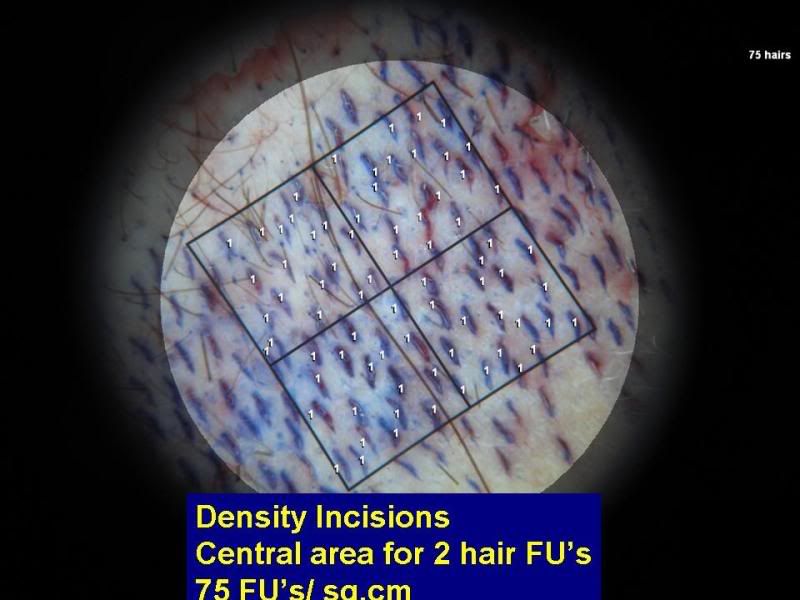
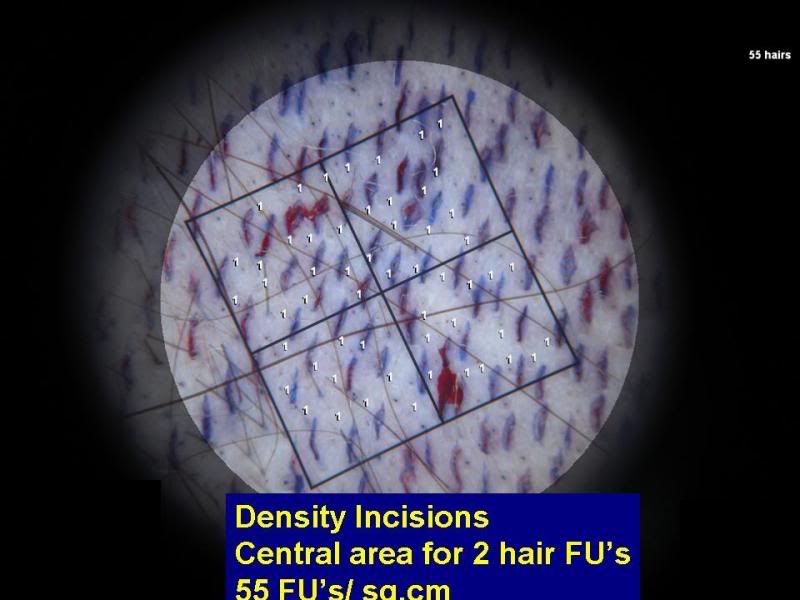
2) We often are transplanting into areas in which there is existing hair in the early stages of thinning. In most of these cases I need to plant 20 to 30 FU/sqcm in these areas to get an excellent cosmetic look. With proper magnification I can plant 30 to 40 FUsqcm in these areas but usually chose not to. I find that in most cases these extra grafts do not yield a significant denser look. Some argue that if we can plant more hair in an area then why don t we do it as a preventative measure. The possible advantage of this preventative philosophy is that as a patient loses his native hair he still has more transplanted hair and will not need another hair transplant? The disadvantage of dense packing in areas of pre-existing hair is that there is an increased risk of transection and shock loss which could damage existing hair. I am not sure the advantage outweighs the disadvantages of this preventative philosophy. Especially because in my experience if a patient does have progressive hair loss they will still want another transplant to achieve their goals and we will not have saved them another hair transplant.
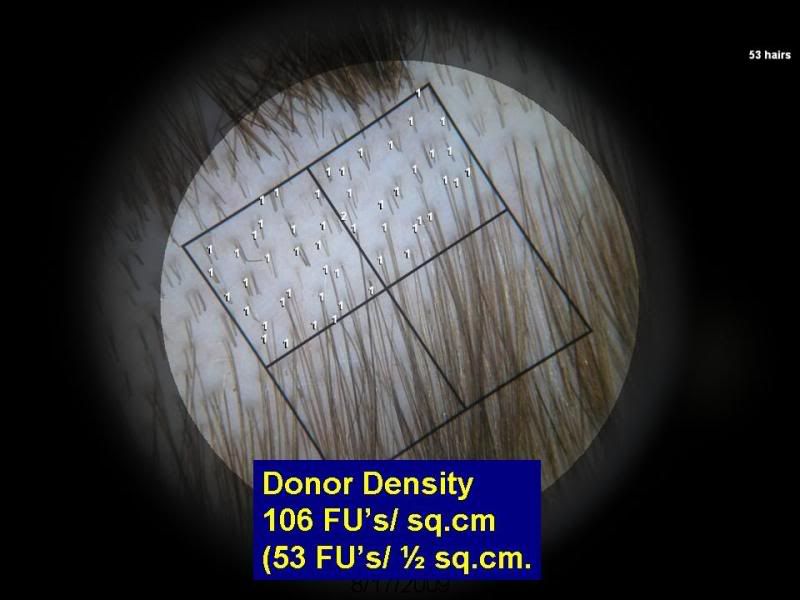
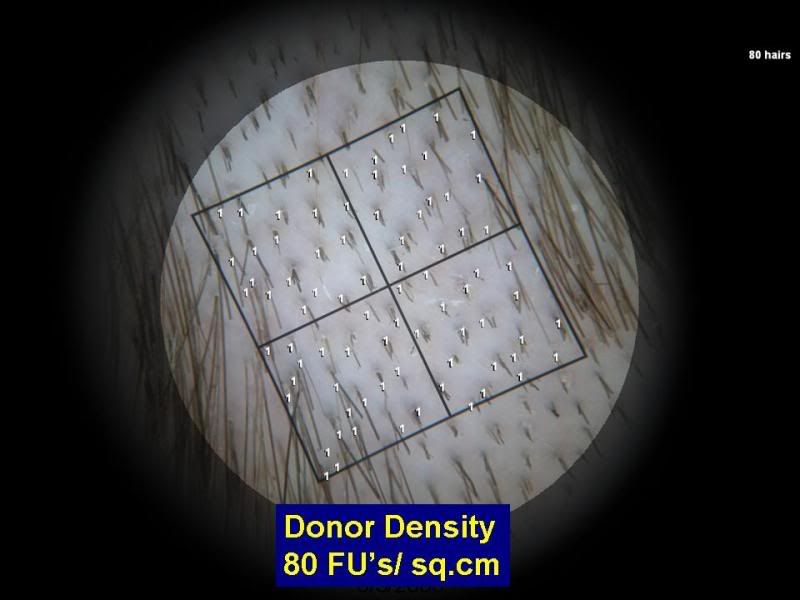
3) All patients have a different percentage of 1,2,3,and 4 hair FU s. There are studies which show that the number of 4 hair FUs can vary from 5% to 20% of the total graft count. It is difficult to compare surgeries without knowing the exact number of 1,2,3, and 4 hair FUs which allows us to calculate the number of hairs transplanted.
There is some discretion when cutting FUs. The photo below is a close up of a patient s donor hair. The area circled in Black is a 3 hair FU that could not be split. But as you can see the area circled in Red can be cut many ways.

At SMG we do believe that the larger 4 and 3 hair FUs give a greater illusion of density in the central core area and thus try to get as many 3 and 4 hair FU unless we are doing a hairline case or the patient has coarse dark hair. There is the possibility that our results look similar to some of the larger cases one sees on the internet because even though we are transplanting less total grafts we are transplanting more hair per graft. Also, by placing the maximum amount of 3 and 4 hair FUs in the central core area we believe we get a greater illusion of density even if we are using the exact same number of total hairs without compromising the naturalness.
If we can achieve the same cosmetic results using fewer grafts I believe there are some potential benefits to the patient. Here are some advantages I can think of:
1) Never lose sight of the basic principle of hair transplant surgery that we are using a limited donor supply to cover a potentially expanding balding area of the scalp. If we can get the same or similar results using fewer grafts, we have more grafts left over for future hair transplants if needed.
2) We strive to get the best graft survival when doing a hair transplant surgery. To maximize graft survival we protect them from dehydration by placing them in physiologic holding solution on ice, use tiny micro blades to limit the amount of vascular trauma to the scalp, and use gentle placing techniques. Most published studies show that even under ideal conditions we do not get 100% graft survival. I still have concerns about surgeries in which the grafts are out of the body for greater then 6 hours. Graft survival decreases the longer the grafts are out of the body. The most commonly sited study shows that after 4 hours graft survival decreases to 95%, after 6 hours graft survival decreases to 90%, and then graft survival continues to decrease by 2% for every additional hour they are out of the body. Also, as the cases go longer there is the possibility of staff fatigue resulting in less careful graft cutting and placing which could decrease graft survival. Taking into consideration that there is the potential for less graft survival as the cases become larger and go longer, I believe there is an advantage to keeping surgeries to the size where the placing can be completed within 4 to 6 hours.
A point I would like to make about graft survival is that we can not accurately measure graft survival in the clinical setting. The published studies on graft survival are done on completely bald scalp, in one centimeter square boxes that are tattooed onto the scalp, and the hair is planted as soon as it is cut. Even in these studies we usually do not get 100% graft survival. The graft survival ranges from 90% to 100%. Taking these studies into consideration no clinic can say they get 100% graft survival. My educated guess is that most good clinics get about 95% graft survival.
In general we judge our hair transplant results by the way the outcome looks. Since in clinical practice we can t accurately measure graft survival, as the sessions get larger we need to decide when the potential risk for decrease graft survival outweighs the benefit of a large session. Here is a hypothetical example to point out the potential risk. Let s say 4,000 and 5,000 grafts are planted in the exact same area. Now let s say the 4,000 transplant yields 95% graft survival and the 5,000 graft transplant yields 85% graft survival. That leaves us 3,800 and 4,200 grafts respectively. The 5,000 graft transplant will still look better then the 4,000 graft transplant even though there is less graft survival. I am not saying this is what happens, but since we can not accurately measure graft survival in our clinical practice the doctor and patient need to decide when this potential risk outweighs the benefits of a large megassesion.
3) Another advantage of keeping the surgery as short as possible is that there is decrease risk of medical side effects. Most patients tolerate the surgery fine, but there are some patients who get nausea, irretraceable hiccups, back /neck pain, or difficulty in keeping the surgical area numb. In my experience I find these side effects are more common during long surgeries. When a patient has these side effects it makes the planting more difficult and can affect graft survival.
4) As the surgeries increase in time, there is the possibility of Deep Vein Thrombosis (DVT). DVT is blood clot in the deep veins in the leg. Prolonged immobilization is one of the risk factors for DVT. A study showed that travelers who are greater then 50 years old have a 10% chance of developing asymptomatic DVT s on airplane flights that last longer then 8 hours. Lancet May 12,2001;357:1485-9 These asymptomatic DVT s usually do not cause any medical problems. But very rarely they can lead to a blood clot in the lung called a Pulmonary Embolism, which is a medical emergency and needs hospitalization. I had such an occurrence on a 45 year old male whose surgery lasted over 8 hours. (I published this case in the Hair Transplant Forum International) Like I said this is a very rare occurrence, but the possibility increases as we increase the length of surgery. When does this risk of DVT outweigh the cosmetic benefits of a prolonged cosmetic surgery?
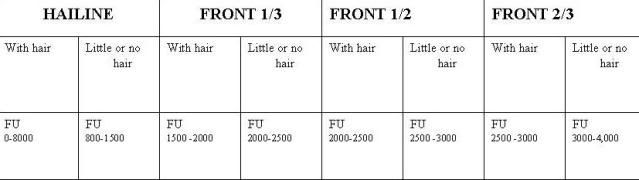
At Shapiro Medical Group we do have general guidelines for the number of grafts we will transplant into different areas of the scalp. The guidelines are printed in the table below. These general guidelines are good for the average patient but sometimes our sessions will go larger and sometimes smaller then in these guidelines.
In summary, how many grafts are needed to get excellent results varies for each patient depending on many factors. But I do believe that if we can get the same or similar results using less grafts there are some advantages. We have less chance of using up limited donor supply that may be needed in future surgeries, potentially increase our graft survival, and limit potential medical risk as much as possible.
Paul Shapiro, MD
We've seen common responses when posting Shapiro Medical Group patients on different ht forums. They usually state how good the case looks considering the small number of grafts we use. Here are a few examples I'm referring to:
This is great result for only 2500 grafts
Amazing coverage for the number of grafts Janna.
janna, a very pleasing result with relatively few grafts(considering the area covered)
Wow, Janna! Those results for the # of grafts are amazing, they really are
These comments suggest that there may be a misconception on the number of grafts needed to accomplish a patient s hair transplant goals. I like to think that we use the appropriate amount of grafts for each case taking into consideration the patients goals, donor density, hair caliber, age, degree of balding, family history, response to medical treatment, and the risk/benefit ratio as the cases get larger and go longer.
I would like to point out a few reasons why surgeries using less grafts may lead to the same or very similar results to transplants using greater number of grafts.
1) Each patient has a threshold level of hair density in which their hair will look full under most conditions. Once this threshold is reached as we increase the hair density we get only minimal esthetic improvement. For example let s say a certain patient needs 2,000 FU to reach this threshold level for the area being transplanted. If we transplant 2,500 FU in this area the esthetic improvement will be very similar to planting 2,000 FU. Thus the results of the two transplants could look similar even though in one surgery 500 more FU were planted.
2) We often are transplanting into areas in which there is existing hair in the early stages of thinning. In most of these cases I need to plant 20 to 30 FU/sqcm in these areas to get an excellent cosmetic look. With proper magnification I can plant 30 to 40 FUsqcm in these areas but usually chose not to. I find that in most cases these extra grafts do not yield a significant denser look. Some argue that if we can plant more hair in an area then why don t we do it as a preventative measure. The possible advantage of this preventative philosophy is that as a patient loses his native hair he still has more transplanted hair and will not need another hair transplant? The disadvantage of dense packing in areas of pre-existing hair is that there is an increased risk of transection and shock loss which could damage existing hair. I am not sure the advantage outweighs the disadvantages of this preventative philosophy. Especially because in my experience if a patient does have progressive hair loss they will still want another transplant to achieve their goals and we will not have saved them another hair transplant.
3) All patients have a different percentage of 1,2,3,and 4 hair FU s. There are studies which show that the number of 4 hair FUs can vary from 5% to 20% of the total graft count. It is difficult to compare surgeries without knowing the exact number of 1,2,3, and 4 hair FUs which allows us to calculate the number of hairs transplanted.
There is some discretion when cutting FUs. The photo below is a close up of a patient s donor hair. The area circled in Black is a 3 hair FU that could not be split. But as you can see the area circled in Red can be cut many ways.
At SMG we do believe that the larger 4 and 3 hair FUs give a greater illusion of density in the central core area and thus try to get as many 3 and 4 hair FU unless we are doing a hairline case or the patient has coarse dark hair. There is the possibility that our results look similar to some of the larger cases one sees on the internet because even though we are transplanting less total grafts we are transplanting more hair per graft. Also, by placing the maximum amount of 3 and 4 hair FUs in the central core area we believe we get a greater illusion of density even if we are using the exact same number of total hairs without compromising the naturalness.
If we can achieve the same cosmetic results using fewer grafts I believe there are some potential benefits to the patient. Here are some advantages I can think of:
1) Never lose sight of the basic principle of hair transplant surgery that we are using a limited donor supply to cover a potentially expanding balding area of the scalp. If we can get the same or similar results using fewer grafts, we have more grafts left over for future hair transplants if needed.
2) We strive to get the best graft survival when doing a hair transplant surgery. To maximize graft survival we protect them from dehydration by placing them in physiologic holding solution on ice, use tiny micro blades to limit the amount of vascular trauma to the scalp, and use gentle placing techniques. Most published studies show that even under ideal conditions we do not get 100% graft survival. I still have concerns about surgeries in which the grafts are out of the body for greater then 6 hours. Graft survival decreases the longer the grafts are out of the body. The most commonly sited study shows that after 4 hours graft survival decreases to 95%, after 6 hours graft survival decreases to 90%, and then graft survival continues to decrease by 2% for every additional hour they are out of the body. Also, as the cases go longer there is the possibility of staff fatigue resulting in less careful graft cutting and placing which could decrease graft survival. Taking into consideration that there is the potential for less graft survival as the cases become larger and go longer, I believe there is an advantage to keeping surgeries to the size where the placing can be completed within 4 to 6 hours.
A point I would like to make about graft survival is that we can not accurately measure graft survival in the clinical setting. The published studies on graft survival are done on completely bald scalp, in one centimeter square boxes that are tattooed onto the scalp, and the hair is planted as soon as it is cut. Even in these studies we usually do not get 100% graft survival. The graft survival ranges from 90% to 100%. Taking these studies into consideration no clinic can say they get 100% graft survival. My educated guess is that most good clinics get about 95% graft survival.
In general we judge our hair transplant results by the way the outcome looks. Since in clinical practice we can t accurately measure graft survival, as the sessions get larger we need to decide when the potential risk for decrease graft survival outweighs the benefit of a large session. Here is a hypothetical example to point out the potential risk. Let s say 4,000 and 5,000 grafts are planted in the exact same area. Now let s say the 4,000 transplant yields 95% graft survival and the 5,000 graft transplant yields 85% graft survival. That leaves us 3,800 and 4,200 grafts respectively. The 5,000 graft transplant will still look better then the 4,000 graft transplant even though there is less graft survival. I am not saying this is what happens, but since we can not accurately measure graft survival in our clinical practice the doctor and patient need to decide when this potential risk outweighs the benefits of a large megassesion.
3) Another advantage of keeping the surgery as short as possible is that there is decrease risk of medical side effects. Most patients tolerate the surgery fine, but there are some patients who get nausea, irretraceable hiccups, back /neck pain, or difficulty in keeping the surgical area numb. In my experience I find these side effects are more common during long surgeries. When a patient has these side effects it makes the planting more difficult and can affect graft survival.
4) As the surgeries increase in time, there is the possibility of Deep Vein Thrombosis (DVT). DVT is blood clot in the deep veins in the leg. Prolonged immobilization is one of the risk factors for DVT. A study showed that travelers who are greater then 50 years old have a 10% chance of developing asymptomatic DVT s on airplane flights that last longer then 8 hours. Lancet May 12,2001;357:1485-9 These asymptomatic DVT s usually do not cause any medical problems. But very rarely they can lead to a blood clot in the lung called a Pulmonary Embolism, which is a medical emergency and needs hospitalization. I had such an occurrence on a 45 year old male whose surgery lasted over 8 hours. (I published this case in the Hair Transplant Forum International) Like I said this is a very rare occurrence, but the possibility increases as we increase the length of surgery. When does this risk of DVT outweigh the cosmetic benefits of a prolonged cosmetic surgery?
At Shapiro Medical Group we do have general guidelines for the number of grafts we will transplant into different areas of the scalp. The guidelines are printed in the table below. These general guidelines are good for the average patient but sometimes our sessions will go larger and sometimes smaller then in these guidelines.
In summary, how many grafts are needed to get excellent results varies for each patient depending on many factors. But I do believe that if we can get the same or similar results using less grafts there are some advantages. We have less chance of using up limited donor supply that may be needed in future surgeries, potentially increase our graft survival, and limit potential medical risk as much as possible.
Paul Shapiro, MD